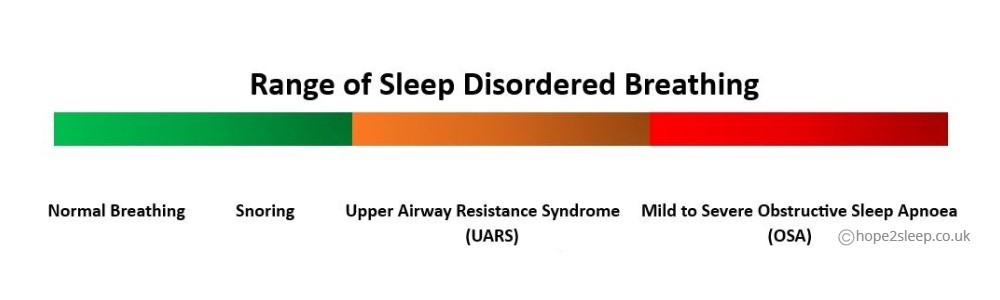
| Upper Airway Resistance Syndrome (UARS)
A less well-known, yet common sleep disorder, is Upper Airway Resistance Syndrome (UARS) and is often the case when people have a sleep study with the results stating too low an AHI (apnoea-hypopnoea index) score to be classed as a diagnosis for Sleep Apnoea. (The minimum criteria for the diagnosis of Sleep Apnoea is an AHI 5). It should be noted that very often UARS does eventually progress into Sleep Apnoea for various reasons, such as ageing and loss of muscle tone in the upper airway, weight gain, the need for sedating medications or regular alcohol use etc. If you haven't had a sleep study to rule out Sleep Apnoea this is advisable first as many people assume they have UARS when it's actually Obstructive Sleep Apnoea (OSA) they are suffering from. Whilst most people with OSA do snore, it is possible to be diagnosed with OSA without snoring. For accuracy, the sleep study should not only use a finger pulse oximeter, as often people with UARS or even OSA do not have regular oxygen desaturations, despite having breathing events. In fact, the August 2021 NICE Guidelines for OSA state "consider respiratory polygraphy or polysomnography if oximetry results are negative but the person has significant symptoms." A sleep study using nasal cannulas is needed and if you are having difficulty getting a sleep clinic referral we do have a sleep study service for diagnosing Obstructive Sleep Apnoea. Sadly, UARS is often not always recognised and people can suffer with just as severe daytime symptoms as someone untreated for Sleep Apnoea! Many people who are sure they have Sleep Apnoea, undergo a sleep study and then get informed they don't have it and are consequently discharged from the sleep clinic and the suffering continues..... There are some sleep clinics though who do treat suspected UARS when patients are symptomatic, affecting their quality of life. Dr Christian Guilleminault was a French physician, pioneer and researcher in the field of sleep medicine who discovered UARS and there is an interesting interview between him and Dr Steven Park. Signs and SymptomsUARS symptoms are very similar to those for Sleep Apnoea and it is just as common in men, women and children. Very often people are of average size or very slim with narrow small jaws. UARS does often appear to be common with Ehler's Danlos Syndrome, POTS (Postural Orthostatic Tachycardia Syndrome) and Hypotension (Low Blood Pressure). Put simply, UARS appears to be Sleep Apnoea without the diagnosis, as UARS sufferers don't actually stop breathing for the minimum of 10 seconds which is classed as an apnoea (no breathing), but they struggle to breathe during sleep and suffer from sleep arousals and unrefreshed sleep. Common Signs & Symptoms:-
Other Signs & Symptoms
CausesSimilar to the causes for obstructive sleep apnoea, but the following tend to be more common in UARS:-
Diagnosing UARSIt is difficult to get a true diagnosis of UARS here in the UK as there are few hospitals that offer the gold standard diagnosis, which is Oesophageal Manometry (Pes) normally carried out by Gastroenterology departments. However, it can be suspected by experienced scoring on a polysomnography sleep study, preferably with RIP bands to record chest movement in order to check for how much effort is being made to try to breathe, as UARS sufferers tend to work very hard to breathe during sleep to prevent oxygen desaturations. A sleep consultant will study the wave forms and other relevant data. A Drug-induced Sleep Endoscopy (DISE) can also be helpful like it can be for OSA. An ENT examination can be very useful to to look for causes of UARS. Here in the UK, we have a leading NHS hospital at the UCLH (University College London Hospitals) Snoring & Sleep Disorders Clinic that specialise in sleep disordered breathing, including UARS. In fact one of the consultants, Vik Veer, from the UCLH explains UARS in the following video:- Some sleep clinics these days are willing to treat people for UARS at their discretion, but here in the UK the National Institute for Health and Care Excellence (NICE) does not offer guidance for the treatment of UARS. In fact it was only in 2008 that they recommended CPAP for Obstructive Sleep Apnoea, so we have to hope things will improve for UARS sufferers soon. Treating UARS
We totally empathise with those of you who are struggling with the symptoms of UARS, and would encourage you to research local services in your area. A sleep study to rule out Sleep Apnoea is advisable, and as previously mentioned, very often when people suspect they have UARS without having had a sleep study, it can actually be Sleep Apnoea they are suffering from. Your GP can refer you to your local sleep clinic or if you are having difficulty getting a referral you can book our private sleep study service at the charity. We would also recommend Dr Park's book 'Sleep Interrupted' where there is a wealth of information on UARS as well as Sleep Apnoea.
|
|












 © 2024 Hope2Sleep - a Registered Charity No.1168089 run by Sleep Apnoea Sufferers, CPAP & Ventilation Users and Sleep Professionals. CALL : 0300 102 9711 | Contact Us | Shop Products | Home VAT Registration No GB269 7550 54  |








